INTRODUCTION
Midwifery in Canada is distinguished by the central role of choice of birthplace in the organization of care and the regulation of the profession. In Ontario, midwives offer the choice of birth at hospital, home, or other community-based settings such as birth centers. Registered midwives are the sole primary healthcare providers who routinely receive education and training to attend home births in Ontario. Our study uses the concept of “At Home with Birth”. It conveys not only that midwives attend births at home but also the way in which home birth inspires confidence and skill in physiologic birth in any setting. James also uses this concept in “Birth at Home—At Home with Birth” to explore the client’s experiences of home birth, where this double meaning is also important.1
Home birth attended by trained and well-equipped midwives has been established as a safe and positive choice for low-risk clients, offering unique clinical and emotional benefits for the birthing individual.2–4 Midwifery clients appreciate the control and personal preferences that home birth provides, with beneficial effects on parent–infant bonding and reduced medical intervention.5,6 Midwives’ satisfaction with their work increases in home environments, where they report enhanced alignment with their professional values. Home environments enable midwives to cultivate an intimate rapport with their clients, encouraging mutual trust and shared decision-making.7,8 Prior experience with home births, whether before or during midwifery education, is a key predictor of a midwife’s proficiency and dedication to home birth practices.9
The International Confederation of Midwives’ Global Standards for Midwifery Education states that midwives should be able to “[f]acilitate normal birth processes in institutional and community settings, including women’s homes.”10 Ontario Midwifery Education Programs (OMEP) prepare students to offer home births through studying evidence and integrating content related to home birth in its preclinical and clinical courses. The comprehensive 4-year program involves one and a half years of academic learning and clinical skills education in simulated settings. Academic learning focuses on sciences, social sciences, and research literacy. In the latter two and a half years of the OMEP, students work alongside practicing midwife preceptors and interprofessional healthcare providers in clinical placements. Weekly case-based tutorials inspired by problem-based learning methodologies are held in tandem with placements. Students explore clinical case studies, do independent research, and check-in about their clinical experiences. Students progressively assume increased responsibility during placements, demonstrating growing competence and confidence. The combination of tutorials and placements prepares graduates for the role of the primary caregiver. The College of Midwives of Ontario (CMO) requires that graduates have attended at least 60 births in total, at least 10 of which are out-of-hospital (OOH) births.11
Canadian midwives demonstrate higher confidence and more favorable attitudes to home birth compared to their American counterparts who do not have required exposure to home birth in their education.12 While midwife-attended births as a percentage of all births in Ontario have increased exponentially since regulation, the percentage of home births has not increased significantly and remains approximately 2% of births in the province.4,13 The rapid increase in overall access to midwifery with a stable home birth rate has resulted in a decreased exposure to home births for most midwives in the province. The percentage of midwifery attended births occurring at home has dropped from 25% in 2004 to 14% in 2021.14 This shift is not surprising given that the normative place of birth in the Canadian society is the hospital. The trend, however, creates a challenge for midwifery educators and students.
While the OMEP aims to equip students for home birth practice, the effectiveness of its curriculum in fostering graduates’ competence and confidence in home birth settings has not previously been evaluated. The goal of this research was to evaluate OMEP graduates’ perceptions of their preparedness for home births and ask for their recommendations. The concept of preparedness was chosen deliberately to convey a sense of readiness rather than completion. The concept leaves open preparedness to provide care as a primary care provider, supported by mentors, and is inclusive of the lifelong learning that is part of “practicing” midwifery. This use of the concept of preparedness aligns with Benner’s stages of clinical competence, which proposes that most graduates enter practice as advanced beginners, able to perform tasks and apply learned principles, but still requiring guidance when navigating new, complex, or high-pressure scenarios.15
METHODS
This study utilizes a mixed-methods approach, collecting and analyzing both qualitative and quantitative survey questions to examine factors that influence preparedness for home births among OMEP graduates. This article reports on the quantitative findings of the survey. Qualitative findings are described in our companion article in this issue. As a research team made up of two midwives who practiced in Ontario for over 30 years and two students in the OMEP program, we were mindful of our own experiences and perspectives on home birth and midwifery education throughout the data analysis process.
Recruitment and screening
Eligible participants graduated between 2018 and 2023 with a Bachelor of Health Sciences (BHSc) in Midwifery from one of three OMEPs: Laurentian University (which closed in 2021), McMaster University, or Toronto Metropolitan University (TMU) (previously known as Ryerson University). The survey link was distributed on flyers that were shared through alumni groups, electronic mailing lists, and social media pages. This study was reviewed and approved by the Research Ethics Board at TMU (REB #2023-225).
Data collection
The survey included scaled and open-ended questions, probing areas from demographics and preadmission experiences to comprehensive accounts of clinical training and practice. Participants had the option to elaborate on open-ended questions through zoom interviews with researchers. Twelve of 74 participants completed their open-ended questions over zoom. Upon completing the survey, participants received $50 (Canadian dollars) as an honorarium.
Data analysis
Quantitative data were analyzed using descriptive analysis on SPSS (IBM SPSS Statistics for Windows, Version 29). Ordinal logistic regression was used to assess associations between graduates’ self-reported preparedness for their role as a primary midwife at a home birth at the time of graduation and a series of independent variables. Preparedness was measured on a four-point ordinal scale, with higher scores indicating greater preparedness. For each model, one category within each independent variable was set as the reference group. Results are presented as odds ratios (OR) with 95% confidence intervals (CI), with p < 0.05 considered statistically significant.
RESULTS
A total of 74 graduates completed the survey; 46% graduated from TMU, 37% graduated from McMaster University, and 18% graduated from Laurentian University. Roughly 40% of participants graduated between 2018 and 2020 (prior to the COVID-19 pandemic), and 60% of participants graduated between 2021 and 2023 (Table 1).
Table 1. Participants’ sociodemographic characteristics (N=74).
| Characteristic | n (%) |
|---|---|
| Age | |
| 18–24 | 4 (5.4) |
| 25–34 | 44 (59.5) |
| 35–44 | 20 (27.0) |
| 45–54 | 5 (6.8) |
| 55–64 | 1 (1.4) |
| Gender | |
| Woman | 70 (94.6) |
| Nonbinary/Genderqueer | 5 (6.8) |
| Identity | |
| 2SLGTBQIA+ | 23 (31.1) |
| Racialized (e.g., Black, Indigenous) | 22 (29.7) |
| Person with Disability | 8 (10.8) |
| Graduating University | |
| Toronto Metropolitan University | 34 (45.9) |
| McMaster University | 27 (36.5) |
| Laurentian University | 13 (17.6) |
| Graduating year | |
| 2018 | 7 (9.5) |
| 2019 | 14 (18.9) |
| 2020 | 9 (12.2) |
| 2021 | 12 (16.2) |
| 2022 | 15 (20.3) |
| 2023 | 17 (23.0) |
Before starting their midwifery education, many participants had firsthand experience with childbirth: 41% had given birth, with over 60% of those experiencing OOH births (Table 2).
Table 2. Experiences attending birth prior to admission in the Ontario Midwifery Education Program.
| Experience Prior to Admission | n (%) |
|---|---|
| Given birth before MEP? | |
| Yes | 30 (40.5) |
| OOH Birth | 19 (63.3) |
| No | 44 (59.5) |
| Attended a birth other than your own before entering the MEP? | |
| Yes | 39 (52.7) |
| No | 35 (47.3) |
| Did you attend an unmedicated/physiologic birth(s) (yours or others) prior to entering the program? | |
| Yes | 33 (44.6) |
| No | 41 (55.4) |
In the clinical portion of the midwifery program, participants identified specific courses that contributed to their understanding and preparation for home births. The first clinical placement course “Normal Childbearing” was most frequently mentioned, followed by “Emergency Skills Workshop,” “Complications and Consultation,” and “Advanced Clinical Skills I” (Figure 1). The hands-on immersive components of courses where students were in the primary or secondary role in home births were highlighted as critical to their training (Table 3). The “Emergency Skills Workshop” was valued for equipping students with crucial competencies for urgent scenarios during a home birth.
Figure 1. Distribution of participants’ recall of home birth education across clinical courses in the Ontario midwifery education program.
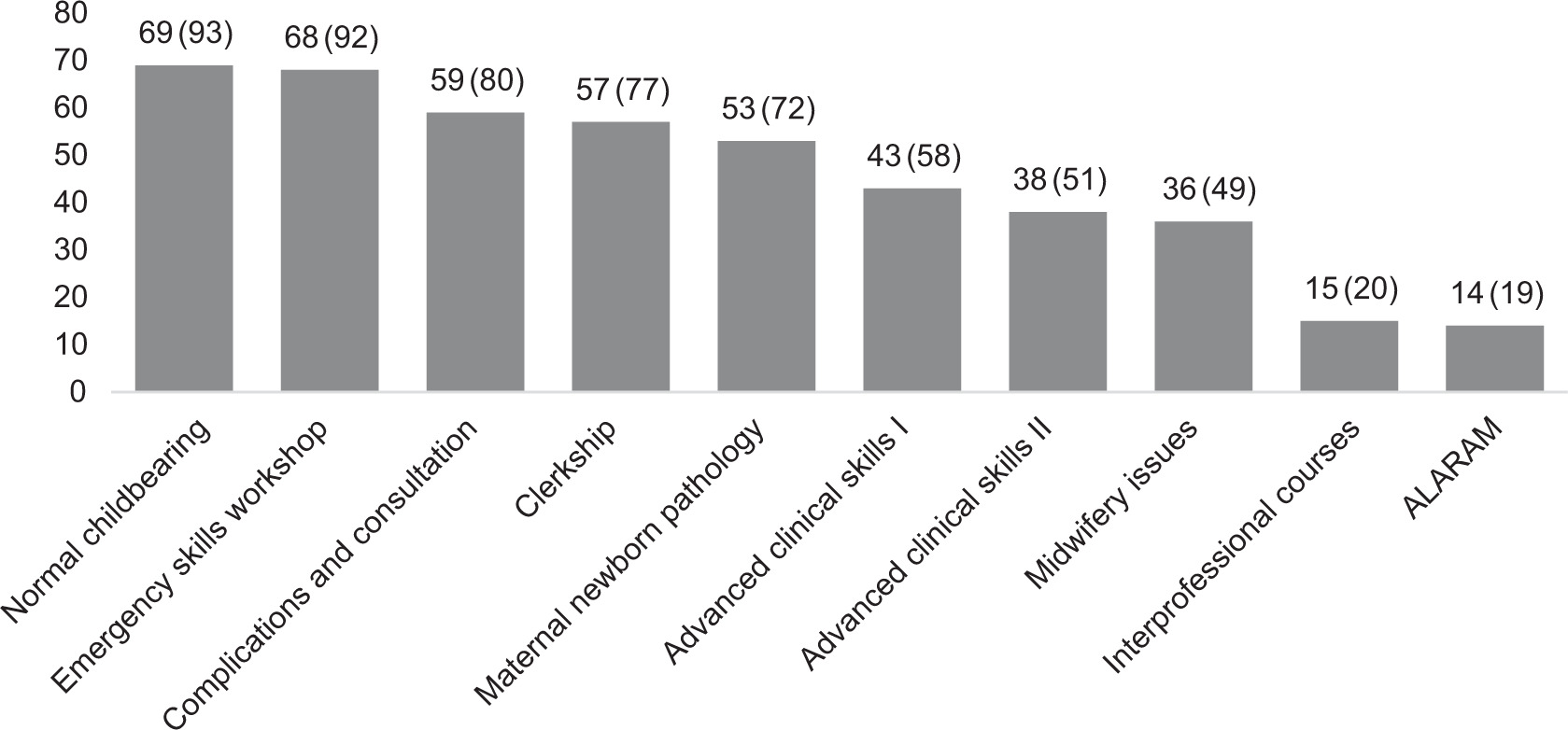
Table 3. Participants’ ranked importance of various factors in preparing for home birth practice.
| How important were the following in helping you feel prepared for home birth practice? | Scale | n (%) |
|---|---|---|
| Attending home births as a student in the primary role | Very important/Important | 74 (100) |
| Less important/Not important | 0 (0) | |
| Attending home births as a student in the secondary role | Very important/Important | 74 (100) |
| Less important/Not important | 0 (0) | |
| ESW course | Very important/Important | 70 (94.6) |
| Less important/Not important | 4 (5.4) | |
| Hands-on demonstration workshops | Very important/Important | 65 (87.8) |
| Less important/Not important | 9 (12.2) | |
| Peer reviews | Very important/Important | 60 (81.1) |
| Less important/Not important | 14 (18.9) | |
| Storytelling by instructors/tutors | Very important/Important | 58 (78.4) |
| Less important/Not important | 16 (21.6) | |
| Case-based clinical scenarios | Very important/Important | 58 (78.4) |
| Less important/Not important | 16 (21.6) | |
| Attending home birth as a student in an observational role | Very important/Important | 57 (77.0) |
| Less important/Not important | 17 (23.0) | |
| Fetal Health Surveillance course | Very important/Important | 44 (59.5) |
| Less important/Not important | 30 (40.5) | |
| Check-in during clinical courses | Very important/Important | 44 (59.5) |
| Less important/Not important | 30 (40.5) | |
| ALARM course | Very important/Important | 40 (54.1) |
| Less important/Not important | 34 (45.9) | |
| Review of Coroner’s Committee on Maternal and Neonatal Mortality Annual Report | Very important/Important | 37 (50.0) |
| Less important/Not important | 37 (50.0) | |
| Presentations by interprofessional lecturers | Very important/Important | 12 (16.2) |
| Less important/Not important | 62 (83.8) |
Despite recalling more coverage of home birth in early clinical courses, tutorials in the later year courses contributed more to participants’ confidence in providing home birth care. Preceptors in both the Normal Childbearing and senior year courses were reported to be key influences, with approximately 80% of participants indicating that their preceptors facilitated both confidence and competence. Case-based clinical scenarios presented during tutorials were rated as “very important” or “important” by 78% of respondents, and storytelling by instructors and tutors was rated similarly (Table 3).
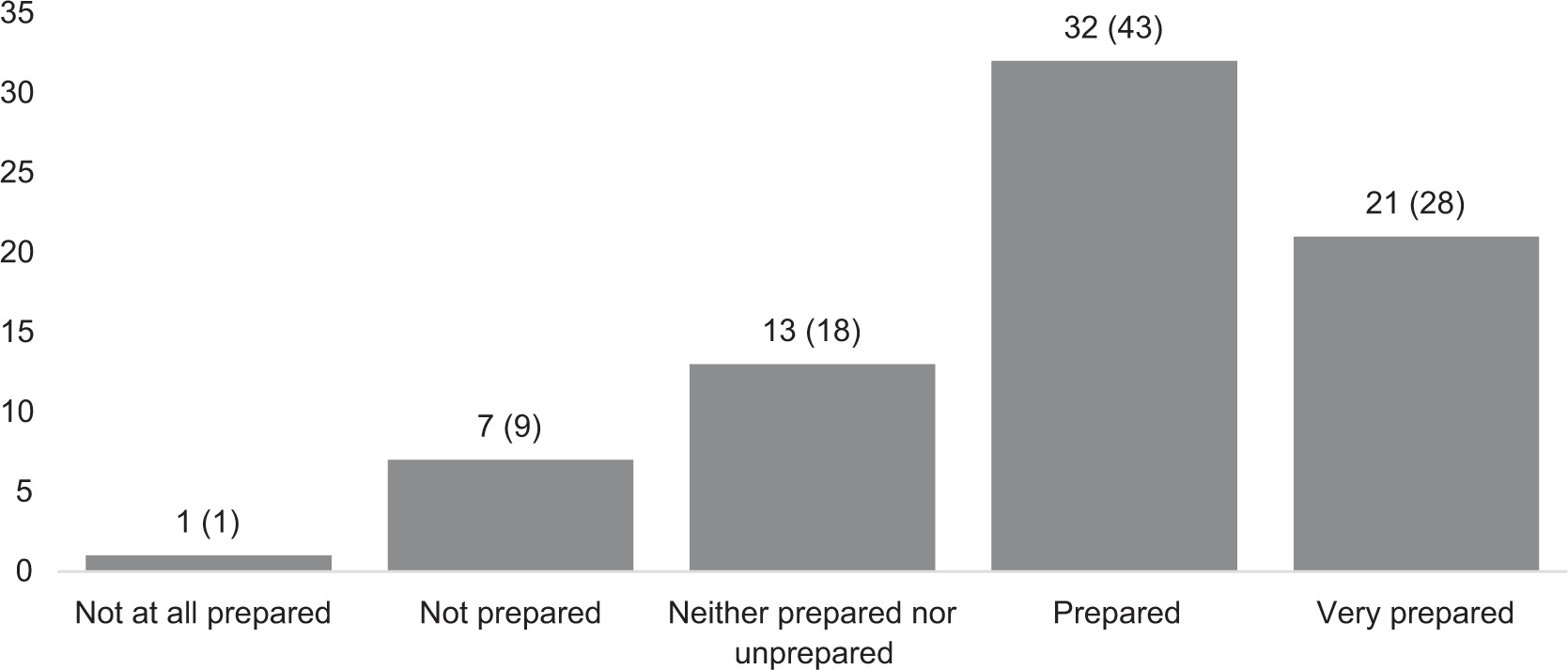
Most participants (71%) felt ready to assume the primary role at a home birth, with 28% “very prepared” and 43% considering themselves “prepared.” Eighteen percent felt neither prepared or unprepared. Ten percent reported feeling unprepared or not at all prepared (Figure 2).
Figure 2. Perceived preparedness of participants to assume the primary role at a home birth upon graduation from the Ontario Midwifery Education Program.
When the number of home births graduates attended in the OMEP was grouped into low (≤10), medium (11–20), and high (≥21) categories (Table 4), those who had higher home birth attendance categories had significantly greater odds of reporting higher preparedness levels compared to those in lower attendance categories (OR = 5.35, 95% CI [2.68, 10.66], p < 0.001). No significant differences in preparedness were found based on age group, school of graduation, graduation year, ethnicity, gender or sexual identity, disability, prior attendance at physiologic births in an OOH setting before entering the MEP, or experience with hospital transports or transfers of care. Although prior attendance was not statistically significant, participants’ reflections tended to indicate these experiences were influential and we report them in our companion article in this issue.
Table 4. Distribution of home birth experience among OMEP graduates
| Total number of home births attended in the OMEP | n (%) |
|---|---|
| ≤10 | 26 (35.1) |
| 11–20 | 31 (41.9) |
| ≥21 | 17 (22.9) |
Graduates who reported supportive preceptors had significantly higher odds of reporting greater preparedness compared to those who did not (OR = 4.09, 95% CI [1.39, 12.00], p = .010). In contrast, whether preceptors in Normal Childbearing facilitated confidence was not significantly associated with preparedness ratings (OR = 1.52, 95% CI [0.54, 4.30], p = .427).
DISCUSSION
Providing choice of birthplace is fundamental, and a midwife’s competence and confidence in OOH settings influences their attitudes and practices.9 This study highlights the interplay between the educational content delivered within the classroom and experiential hands-on learning, both of which are critical in preparing midwives for the realities of home birth care. The results provide insights into how midwifery education can be optimized to align with professional standards, student needs, and the evolving healthcare environment in Ontario.
Most participants in this study, 71%, reported feeling ready to assume the primary role at a home birth upon graduation. A key strength identified in this study was the early introduction of evidence-based research supporting the safety and benefits of home births, and participants consistently highlighted the importance of learning about home births through academic content, such as research studies, case studies, and resources by midwifery organizations. These evidence-based foundations not only dispelled misconceptions about the risks of home births but also built confidence by normalizing the practice as a viable option for low-risk clients. Emergency skills were particularly valued by participants. These workshops provided students with hands-on training in managing critical situations, and participants emphasized that the confidence gained through these courses was integral to their ability to provide safe care in an OOH setting. This finding is reinforced by recent research from a systematic review about midwives experiences of emergencies in community settings.16
Midwifery practice groups that maintained a positive outlook toward home birth and provided opportunities for students to participate in home births also played a pivotal role in enhancing graduates’ preparedness. This aligns with studies among American and Norwegian midwives, which show that exposure to home or other OOH births through clinical rotations and mentorship fostered positive attitudes toward home birth, increased willingness to offer this choice to birthing parents, and was essential to perceiving birth as a natural process rather than a pathological one.9,17 Not surprisingly, the higher the number of home births attended the more confident graduates were.
Mentorship through preceptors was a critical factor in preparing graduates for home birth practice. These mentors bridged the gap between theoretical learning and practical application, reinforcing trust in home birth as a safe and viable option for low-risk clients. This reflects Situated Learning Theory, which posits that learning occurs most effectively when embedded in authentic, socially situated contexts, where novices engage in legitimate peripheral participation and gradually become integrated into a community of practice.18 By engaging in real-world OOH birth settings under the guidance of skilled mentors, students gradually moved from peripheral observation to full participation, developing both competence and confidence.19 This finding is echoed by Zwedberg et al., who identify that good preceptorship is characterized by the preceptor’s self-efficacy and their capacity to nurture student confidence and independence, underscoring the critical impact of skilful mentorship on midwifery education outcomes.20
A smaller proportion of participants, roughly 10%, expressed a lack of readiness to be a primary care provider at a home birth upon graduating from the OMEP. An additional 18% reported feeling neither prepared nor unprepared, a finding which is perhaps consistent with Benner’s levels of competence with graduates as “advanced beginners”.15 Participants reported that home birth education was often treated as ancillary rather than integral to the curriculum. While the program covered the safety and benefits of home births, the overall coverage of home birth topics was tutor-dependent and for some minimal, leaving them to feel underprepared for the realities of home birth practice. In addition, senior year courses focused heavily on preparing students for complications and medical interventions. Workshops like the Emergency Skills and annual Neonatal Resuscitation training, though invaluable for teaching critical emergency management skills, were cited as primary resources for learning about home birth. It is important to note that while these workshops provided vital preparation for worst-case scenarios, some participants noted in answering the short answer questions that a focus on complex care overshadowed discussions of normal uncomplicated home births, a nuance that we will discuss in the companion article.
Implications for practice and policy
Findings from this study highlight opportunities to build on and strengthen the integration of home birth education to address gaps and support the development of competent and confident midwives.
The OMEP curriculum was developed at a time when home births represented a higher percentage of births in midwifery practices. With exponential growth of the profession over the last three decades and less consistent exposure in the clinical setting, a more intentional approach to embedding OOH birth education throughout the curriculum and clinical training opportunities is essential. Introducing physiologic birth workshops early in the program and ensuring continuing exposure throughout the program could balance the necessary focus on emergencies. Incorporating instructional strategies, such as increased case-based reviews and clinical check-ins in tutorial specific to OOH settings, could provide students with greater theoretical grounding. These could cover topics such as identifying suitable candidates for OOH birth and understanding its safety, lower intervention rates, and high satisfaction.
Tutors and preceptors both played an important role. Our findings support increasing resources for tutors and preceptors, providing guidance on effective teaching strategies, navigating informed choice and risk conversations, and modeling client-centered care in OOH settings. OMEP preceptor meetings and workshops could provide a platform for sharing resources for best practices, addressing common challenges, and fostering a consistent approach to mentorship for physiologic birth and home birth, even when clinical experiences are limited. A study with midwifery preceptors in Alberta by Upadhyaya et al. found that targeted training enhanced mentorship practices, supporting preceptors in bridging the gap between theoretical learning and clinical application.21 The OMEP and the Association of Ontario Midwives (AOM), in consultation with preceptors, could develop practice guidelines, share tools, and offer workshops to support OOH education for midwifery practice groups. On a larger scale, support for confidence and competence among midwives to support and teach about physiologic birth across settings could be integrated into ongoing professional development and peer-learning opportunities frameworks through the Canadian Association of Midwives (CAM).
Systemic changes are also vital to sustain and expand OOH learning opportunities. Data from the BORN data registry reveal high variation between midwifery practices in rates of home birth across the province, ranging from 2 to 53%. Rates of transfer of care in labour from midwives to physicians also vary significantly from practice to practice (6–51%) (22). Both of these variations can impact students’ learning opportunities, competence, and confidence. Strengthening regulatory and healthcare environments could empower midwives in offering and advocating for OOH births and more broadly for physiologic birth. Efforts could include improving interprofessional communication and collaboration, developing respectful transfer protocols, and ensuring institutional policies align with midwifery-led care principles.23 Advocating for additional birth centers and exploring funding models that incentivize OOH births specifically and physiologic birth more generally may provide midwives with the resources and support necessary to confidently offer home birth as a safe option with many benefits. Regular audits by practices or by the CMO of rates of OOH birth, intervention rates, and transfer practices in midwifery practice groups could also identify the most effective ways to support midwives in providing choice of birthplace and quality midwifery care.
Strengths and limitations
Drawing from a cohort of 74 graduates from OMEP, this study captures a range of perspectives on the preparedness for home birth practice. However, several limitations should be noted. First, the voluntary nature of recruitment may have introduced self-selection bias, as individuals with a strong interest in or with favourable views toward home birth may have been more inclined to participate. Notably, among participants who had given birth themselves, more than half had experienced a home birth, indicating a potential skew in the sample toward those with a personal preference or familiarity with OOH birth. Second, while participants were drawn from all three OMEPs and analysis did not show a significant difference in preparedness related to institution, our findings may be influenced by program-level differences in how home birth is approached within each institution. Variability in curriculum design, faculty emphases, and clinical placement opportunities may have shaped participants’ educational experiences in distinct ways, limiting the generalizability of findings. Notably, our study period included participants whose education would have been impacted by the COVID-19 pandemic. Future research will explore whether there are differences in perspectives from those whose midwifery education was prior to or during the pandemic. Finally, the study reflects the context of midwifery education and practice in Ontario and may not be fully transferable to other provinces, territories, or countries with different educational frameworks, regulatory structures, or healthcare systems.
CONCLUSION
This study provides the first focused examination of OMEP graduates’ perceptions of their preparedness for home birth practice. While most graduates felt ready to assume the primary role at a home birth, preparedness was strongly shaped by the quantity and quality of their home birth exposure during training, as well as the confidence and modelling offered by preceptors. These findings underscore that experiential learning, particularly repeated, meaningful participation in out-of-hospital (OOH) births, is central to developing both competence and confidence.